

Minnesota Department of Health A Framework of Ethics for Monoclonal Antibodies Allocation During the COVID-19 Pandemic:
Noting that those who do not have “BIPOC status”, which is basically, non-Hispanic whites, would be considered “deprioritiz.”[ed]It is based solely on the patient’s race and ethnicity. An elderly white person with the exact same health and age would have priority over an otherwise wealthy patient.
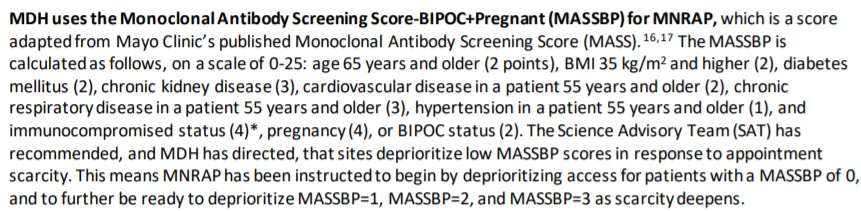
This is the Department’s reasoning:
This score was developed in consultation with Mayo Clinic, University of Minnesota, and Mayo Clinic. It specifically examined the importance of including BIPOC and pregnancy status when examining poor clinical outcomes. UMN found, in an analysis of 41,000 patient records, that both pregnancy and BIPOC status, after accounting for other covariates, were independently associated with poor clinical outcomes from COVID-19 infection….
FDA acknowledged that, in addition to some underlying conditions, patients may also be at risk of severe COVID-19 progression. FDA acknowledged that eligibility determinations for mAbs may include race and ethnicity, in addition to other health conditions. Ethically, it’s appropriate to take into account race and ethnicity for mAb eligibility determinations when there is an increased risk of poor COVID-19 outcomes of Black, Indigenous and Other People of Color (BIPOC) populations. The FDA acknowledges that eligibility cannot be determined based solely on underlying conditions. MDH found this risk in the current data. Health systems need to consider potential risks associated with race and ethnicity in deciding whether individuals are eligible for mAbs. But it’s always true that healthcare providers should consider “the benefit-risk” for every patient.
As I noted in my post about the New York COVID race discrimination scheme, this is unconstitutional: Use of race as a proxy for supposed greater risk—instead of focusing on the more directly relevant factors (“race-neutral alternatives,” in doctrinal terms), such as underlying medical conditions, vaccination status, lack of access to good alternative care, or the like—would violate the Equal Protection Clause in this situation. If the Department has concerns about underdiagnosis, it might provide funding to ensure that all eligible patients receive proper diagnosis. However, this cannot be done by relying on being Hispanic or non-white as an excuse for such underdiagnosis. To quote Judge Amul Thapar in Vitolo v. Guzman (6th Cir. (Cir.
These are the harsh realities of the Small Business Administration’s racism-gerrymandering. Imagine two childhood friends—one Indian, one Afghan. Each of them own restaurants and have both suffered severe losses from the pandemic. In the event that both applicants apply for the Restaurant Revitalization Fund the Indian applicant will in all likelihood be given priority over his Afghan counterpart. Why? It is because of his ethnic heritage. To divide us by race is indeed “a terrible business.” This is a violation of the Constitution by the government.
This logic could be applied even more strongly, I believe, if government officials explicitly discriminate based on race or ethnicity, not only in funding, but also in access to lifesaving drugs.
Although the Court did not rule out the possibility of using a proxy in exceptional circumstances, when it was genuinely impossible, race or ethnicity may be used in medical care. There seems little evidence to support this, given the heterogeneity of the “BIPOC”. For instance, the Department cites the FDA document to justify its anti-BIPOC discrimination. It then indirectly relies on the CDC document (Obesity/Ethnicity and COVID-19), through one of the few references to race.
Obesity Worsens Outcomes from COVID-19 …
Obesity has a disproportionate impact on certain racial and ethnic minorities groups
The 2018-2020 combined data show significant racial/ethnic disparities
Non-Hispanic Black adults were the most obese (40.7%), followed by Hispanic adult (35.2%) and non-Hispanic White adults (30.3%) and non-Hispanic Asian adults (11.6%).
Hard to see how there would be any reason to think that “BIPOC” status as such—combining blacks, Hispanics, Asians, and American Indians of all backgrounds and economic status—is going to offer a consistent picture of any otherwise unmeasurable variables. The “BIPOC” status of this Minnesota government department is not a choice between the groups it prefers and those to which it wishes to “deprioritizing” access.
Thank you to Hans Bader, and John Hinderaker (PowerLine), for this tip.